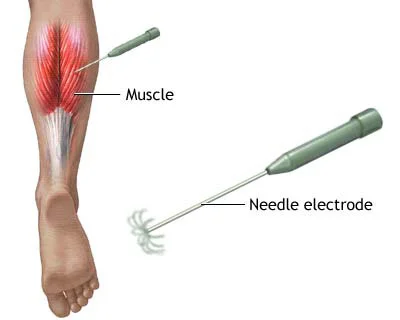
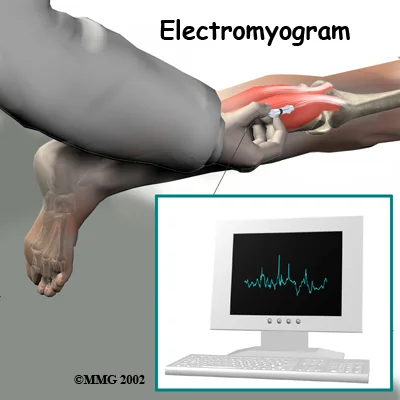
Electrodiagnostics (EDX) testing is used to evaluate the integrity and function of the peripheral nervous system (most cranial nerves, spinal roots, plexi, and nerves), NMJ, muscles, and the central nervous system (brain and spinal cord). EDX testing is performed as part of an EDX consultation for diagnosis or as follow-up of an existing condition. EDX studies can provide information to:

There are many clinical situations where good medical management requires repeat testing, such as in the following examples:
Repeat EDX consultation is therefore sometimes necessary and, when justifiable, should be reimbursed. Reasonable limits can be set concerning the frequency of repeat EDX testing per year in a given patient by a given EDX consultant for a given diagnosis. The following numbers of tests per 12-month period per diagnosis per physician are acceptable:
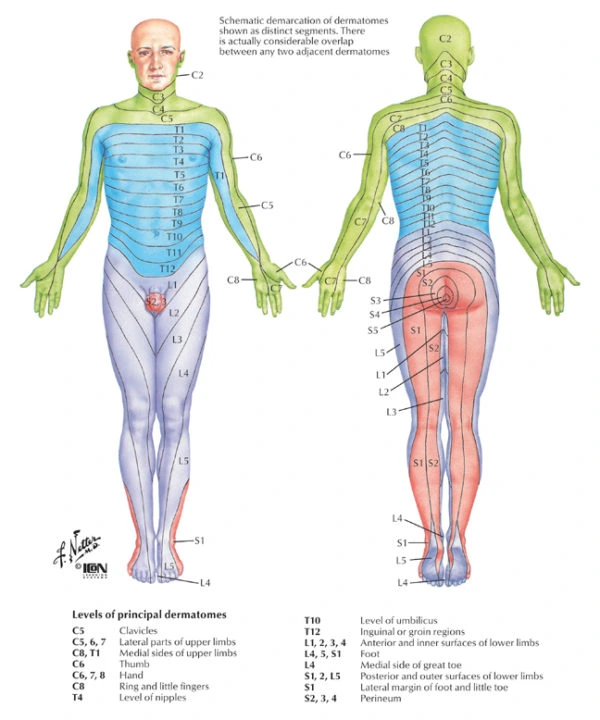
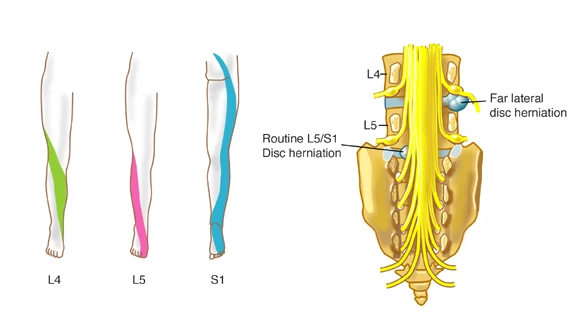
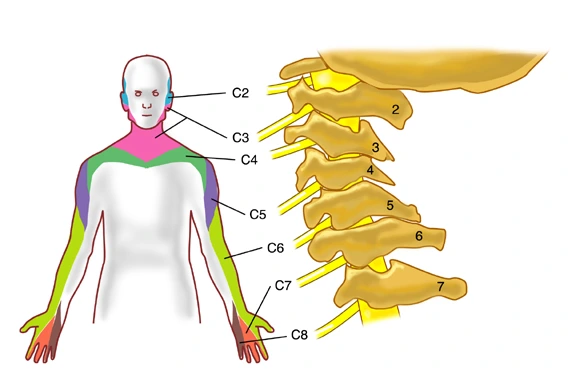
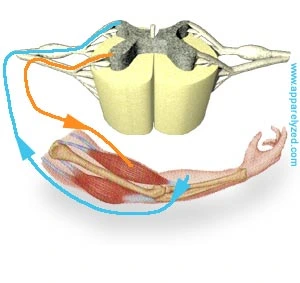
Spinal nerves have motor fibers and sensory fibers. The motor fibers innervate certain muscles, while the sensory fibers innervate certain areas of skin. A skin area innervated by the sensory fibers of a single nerve root is known as a dermatome. A group of muscles primarily innervated by the motor fibers of a single nerve root is known as a myotome. Although slight variations do exist, dermatome and myotome patterns of distribution are relatively consistent from person to person.
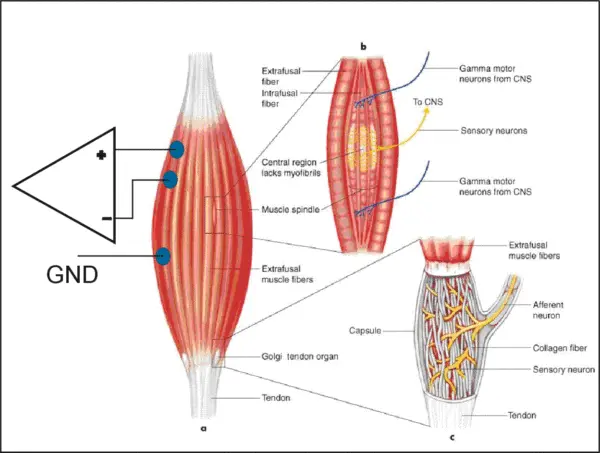
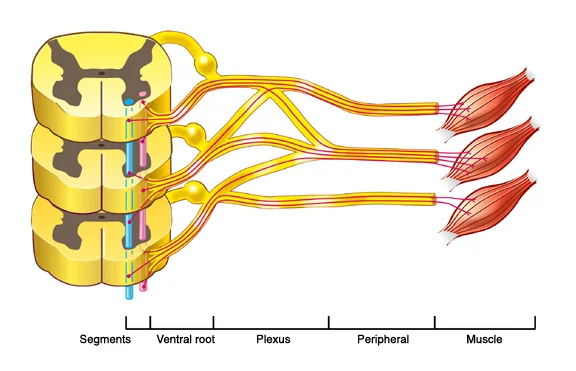
The ventral (anterior) gray matter of the spinal cord contains nerve cells that send axon fibers out, through the nerves, to their end points on the muscles that they activate. Sensory information from the body and arriving instructions from the brain all cause movement by giving instructions to these “motor neurons” in the spinal cord gray matter.
Each muscle in the body is supplied by a particular level or segment of the spinal cord and by its corresponding spinal nerve. The muscle, and its nerve make up a myotome. This is approximately the same for every person and are as follows: